
Gestational Surrogacy for Beginners
An Overview of the Process and Costs of Gestational Surrogacy in the United States
Many of you are aware of how Aaron and I met as teenagers. (If you are new the site, and you are interested, you can catch up on some of it here and here.) This year, we will officially celebrate our 17 year anniversary, though figuring out the exact timetable is always difficult since we met 21 years ago, knew we were going to spend the rest of our lives together, never dated anyone else, and were inseparable. There’s no one date we can point to and say, “This is when we began”. My story is his story. His story is my story. From the time we were teenagers, there was only us. We built our lives, our businesses, our investments, and our home together, hand in hand, moment by moment, day by day, year by year.
We’ve always known that someday we wanted to become parents. Both of us were lucky to come from fairly large families – before the blog went more private as it became necessary to protect our personal lives, it wasn’t unusual to post pictures celebrating the birth of our newest niece or nephew, show you what we were making for Thanksgiving dinner, or celebrate Christmas morning with you. When we began to seriously discuss coming out of what amounted to early retirement, divesting many of our private operating businesses, and launching our new global asset management firm, Kennon-Green & Co., we also decided that the moment had arrived when we were ready to become fathers. Aaron took the lead in gathering research and putting together a roadmap of our options, freeing me to prepare the early regulatory work on the investment group.
Last spring, during a business trip to Chicago, we made several life-altering decisions. One, as you know, was that we were going to part with our equity ownership of our letterman jacket awards company. We wanted no distractions and needed to devote all of our focus to the new adventure in front of us. Two, we decided that we were going to go forward with gestational surrogacy, having children as soon as reasonably possible. We ultimately decided that we’d like to have four kids, possibly two boys and two girls, though that isn’t exactly within our control (it’s possible one or both of us may produce only boys or girls).
Given how much information you’ve shared with all of us over the years, and how generous the people at the gestational surrogacy conference were, I thought it might be good to put together an overview of what we’ve learned about the process during our own journey. Specifically, I wanted to try and provide a high-level answer to a few questions:
- What is gestational surrogacy?
- Who is likely to use gestational surrogacy?
- Why would someone choose gestational surrogacy instead of adoption?
- How does gestational surrogacy work?
- How much does gestational surrogacy cost?
- What are some of the things to consider when undertaking a gestational surrogacy journey?
My hope is that this will make the process a little easier to understand, and a little less overwhelming, if you or a loved one are considering it.
First, let’s tackle the top question on that list.
What Is Gestational Surrogacy?
Gestational surrogacy is a process in which “Intended Parents” (frequently called “IPs”) work with a fertility clinic to create embryos that are their own genetic offspring. The Intended Parents then temporarily entrust their embryos to an altruistic woman who has no genetic relationship to the embryos but who wants to help them build their family. This woman, who is known as the “Gestational Carrier”, agrees to have the embryos implanted into her uterus, where they can grow into healthy babies over the course of nine months. After the babies are born, she returns them to their genetic parents, the Intended Parents.
For example, imagine a husband and wife, John and Lauren. They are happily married. Earlier in life, Lauren had a medical scare and, as a precaution, her doctors recommended a total hysterectomy. Knowing they would someday want to be parents, John and Lauren decided to freeze Lauren’s eggs so they could still have biological children at some point in the future. The couple works with an IVF clinic to combine John’s sperm with Lauren’s eggs to create embryos that are their genetic children. John and Lauren are the Intended Parents. Once they are ready, John and Lauren work with a gestational surrogacy agency to find a woman who will be their Gestational Carrier. Let’s call her Emily. Emily agrees to have one or more of John and Lauren’s embryos implanted into her uterus for nine months, during which she will protect and nurture the baby or babies as they develop. When the baby or babies are born, Emily returns them to John and Lauren, the genetic parents.

How Is Gestational Surrogacy Different from Traditional Surrogacy?
Gestational surrogacy has only been around for a few decades thanks to advances in modern medicine. Before gestational surrogacy existed, there was a different type of surrogacy arrangement that is now known as “traditional surrogacy”. Under a traditional surrogacy arrangement and prior to the age of technology, if Lauren were infertile, John would have slept with Emily, conceived a baby with her, and then Emily would have given the baby to John and Lauren to raise after giving birth. Under a traditional surrogacy arrangement in today’s world of contemporary science, John’s sperm would have been combined with Emily’s egg in an IVF laboratory and then, once the embryo developed, implanted into Emily. Emily would have given the baby to John and Lauren to raise after giving birth.
Traditional surrogacy has been around for as long as humanity existed and from time to time creates moral panics about women selling their babies. For example, in the 1980s, there was a famous court battle, known as the Baby M case, involving a holocaust survivor and his wife. The couple felt compelled to build their family because the husband’s other family members had been killed in the holocaust during the Nazi era, making him the last remaining survivor of his bloodline. The wife was able to have children but suffered from multiple sclerosis and was frightened of the health risks of getting pregnant. They entered into a traditional surrogacy arrangement. The husband’s sperm was combined with another woman’s egg. The other woman then had the resulting embryo – of which she was the biological parent, too – implanted into her uterus. Upon giving birth, the other woman gave the baby to the couple but, shortly thereafter, demanded the child be returned.
In a traditional surrogacy arrangement, the surrogate is not known as a “Gestational Carrier” but, instead, a “Surrogate Mother” because she is also the biological mother of the child. Traditional surrogacy has fallen out of favor in the developed world. Unfortunately, those with an activist agenda, or members of the media who are not aware of how gestational surrogacy works, frequently refer to a Gestational Carrier as a Surrogate Mother when it is both legally and medically inaccurate. In fact, traditional surrogacy is so rare in most countries these days that if you see an article that uses the phrase “Surrogate Mother”, the odds are overwhelming that the journalist is either completely ignorant about the topic he or she is covering, or the writer has a political agenda and is trying to manipulate you. Pay attention to it and you’ll notice that it’s being done purposefully with the hope that you don’t know the difference.
Who Is Likely to Use Gestational Surrogacy?
Gestational surrogacy is most likely to be used by an opposite-sex married couple (husband and wife) due to the inability of the wife to carry the child safely or a same-sex male married couple (husband and husband) due to the lack of a uterus despite being otherwise fertile. Finally, as with adoption, single men and single women sometimes decide to become a parent through gestational surrogacy.
For example, the media has been closely following the gestational surrogacy journey of Kayne West and his wife, Kim Kardashian West. The couple had to use a Gestational Carrier for their third child because, despite the fact they are both fertile, Kim suffers from a condition called placenta accreta, which can be life-threatening. Instead, their biological child, a daughter, was created as an embryo through IVF by combining his sperm and her egg, then implanted into the Gestational Carrier who carried the baby to term for them before returning her to her rightful parents. Elton John and his husband, David Furnish, had their children through gestational surrogacy. The world’s highest-paid athlete, soccer star Cristiano Ronaldo, has three children through gestational surrogacy.
Why Would Someone Decide on Gestational Surrogacy Instead of Adoption?
To answer this question, I am going to have to get personal. I hope you don’t mind. Before I do, though, allow me to get something off my chest.
Aaron and I were willing to adopt and might still choose to adopt in the future. It is an option that has always been on the table and one that we in no way reject. We have family members who grew up in families that had both biological and adopted children and who have discussed adopting. While we only plan on having four kids, it’s entirely possible that twenty years from now, we’ll be like one of our investing heroes, Charlie Munger, and end up with a large number of children. (You think I’m kidding but if that ever happens, you can take it to the bank that we’ll be staging Kennon-Green family musical productions, complete with costumes and lighting.) We have the resources to support them, we love being part of a huge family, and we would love our adopted children as much as we would love our biological children. For heaven’s sakes, we have more godchildren than almost anyone else we know. We love kids. We can’t wait to be parents.
Still, this is one of those questions that I find maddening not because it isn’t a good question – it is, particularly from a public policy perspective – but because:
- It is unfairly applied in the most discriminatory way. This question is practically never asked to straight couples who can get pregnant without a problem. People who would be horrified to walk up to a pregnant woman and ask, “Why didn’t you adopt, instead? You’re so selfish for wanting to have a baby.” will think nothing of doing the same thing to a straight couple or a gay couple using a Gestational Carrier. It’s as if all common sense, decency, compassion, and tact fly out the window. The answer should be blindingly obvious: there is nothing about being a straight couple that has fertility issues, or a gay couple that lacks a uterus, that suddenly makes you more or less likely to desire biological children than anyone else. In fact, I think nobody has a legitimate right to ask this question unless he or she 1.) has no biological children of their own, 2.) has adopted children, and 3.) asks this question to all couples, including perfectly fertile straight couples who have biological children. Then, and only then, are they being consistent in their worldview and standards.
- It demonstrates an appalling, almost offensive, lack of understanding about both the adoption process and the state of LGBT rights in this country. While we’ve come a long way, Obergefell did not solve everything. The Supreme Court has still refused to name sexual orientation a suspect class while, almost comically, acknowledging in its majority opinions about sexual orientation that it is the single most targeted intrinsic characteristic in American history when it comes to state-level legislation and constitutional ballot initiatives that seek to remove protections and rights. Most people are too busy with their lives to pay attention. That’s understandable. Humans are humans and usually only focus on what helps or harms them at any given moment. For example, did you know what the big priority of the Georgia Senate was this week? Take a guess. Give up? It was passing a law that gives adoption agencies the right to refuse to place children with gay married couples. I’m not kidding. The bill is called SB 375 if you care to research it. Not that long ago, right over the border from my hometown, the Governor of Kansas issued an executive order protecting adoption agencies that refused to allow gay couples to adopt. Here in Missouri, such a measure was bound for a constitutional referendum until Democrats launched a 39-hour filibuster and, by some miracle, managed to put it on ice, most likely temporarily. International adoptions? Those are largely out, too, as entire countries ban married gay couples from adopting. Yes, it is possible to do it. Yes, couples do it all the time. However, it is, if you’ll forgive my language, one hell of a mixed signal to be constantly beat over the head with questions about why you don’t adopt then pick up a newspaper to discover that society is trying to further strip away your right to adopt. On top of this, adoption, like gestational surrogacy, is also incredibly expensive, can involve far less certainty than having a biological child (e.g., the birth mother wants to rescind the adoption), poses increased challenges (a substantial percentage of children in the adoption system, understandably, have severe medical and behavioral needs), and involves a maze of legal complexities.
That said, why did we – Joshua Kennon and Aaron Green – decide to go with gestational surrogacy, especially if we may still decide to adopt at some point in the future? There were several reasons. The practical aren’t hard to figure out … as far as genetics go, we hit the jackpot so it seems foolish not to give our children that same advantage. Beyond that, though, it’s something more powerful. I find it difficult to put this into words but I’ll give it my best attempt. Forgive me if I stumble. It’s really more of a feeling than something I can encapsulate into a sentence.
I grew up knowing some of my great grandparents. Over time, I’ve watched the older generations pass away. Today, there are only three remaining family members alive in my grandparents’ generation and then, it’s my parents’ generation that steps up to the final line before the grave, pushed on by the tyranny of time. There will come a day, when I am 80 or 90 years old, when I haven’t heard my mother’s laugh in decades. Maybe, if I’m lucky, and even if only for a moment, I’ll be able to see her when one of my children or grandchildren smiles.
If something were to happen to Aaron before me – the man I have loved since we were children ourselves and with whom my biggest fear is that even though we may be fortunate enough to have a lifetime together, it still won’t be long enough – maybe, if I’m lucky, I’ll be able to see his eyes in our sons or daughters. It might make the pain of losing him more tolerable. The world is more beautiful because he is in it. I want him to leave a piece behind when he goes.
Right now, as I write this to you, I am a miracle. You are a miracle. The atoms that make up our bodies were forged in distant stars at the birth of the universe. Those atoms eventually became life. From that earliest single-cell organism to today, over eons, an unbroken chain has been fastened. That chain is part of the tapestry of existence itself. It includes the hopes, dreams, fears, struggles, and joys of millions of lives that neither of us will ever know but that right now, in this moment, runs through our veins and combines to make us who we are. In my case, I have been entrusted, as the last member that line, with a specific sequence of genes. The odds of me existing in the first place are so incomprehensibly minute that it’s impossible for the mind to grasp. Yet, here I am, a living trustee who will someday fade and be returned to the soil from whence I came. I was gifted life through no virtue or effort of my own. I did nothing to deserve it. It is both an honor, privilege, and moral duty to continue that chain, unbroken. I will not let it die with me. Long after I am gone, and long after my name has been forgotten, I will have repaid my ancestors for the sacrifices they made and paid it forward to those who will never thank me. Through me, they will live on.
…
Enough of that. This was supposed to be an article about the process of gestational surrogacy, not a confessional where I bare my heart to you. Let’s get back to the program.
How Does Gestational Surrogacy Work? A Look At A Typical Gestational Surrogacy Journey
Aaron and I are in the middle of experiencing the gestational surrogacy journey as a married same-sex male couple. Accordingly, this overview is provided from that perspective but it is largely the same for married opposite-sex couples. Broadly speaking, the gestational surrogacy journey works like this:
- Find the egg donor or sperm donor if one of those is missing and can’t be contributed by an Intended Parent
- Find the IVF clinic with which, and the fertility doctor with whom, you want to work when creating your embryos
- Find the gestational surrogacy agency you want to use and enter into an agreement so the staff can start looking for a Gestational Carrier
It’d be best if we take these steps one at a time. That way, it will help you understand what each entails.







Finding an Egg Donor to Create the Embryos
With a married opposite-sex couple, the sperm and the egg usually come from the husband and wife unless there is something that prevents them from contributing it. For us, the technology isn’t there, yet, though there is a good chance that within the lifetime of most people reading this paragraph, it will be possible for two men to have a baby without an outside egg donor. This is because men carry both an X and a Y gene in their DNA and certain advances within stem cell research make it likely that a sample of a man’s skin could be used to reverse-engineer an egg within a laboratory, creating an egg as if he had been female (this is an oversimplification – the actual science that is likely to lead to this result is much more complicated but you get the idea). Aaron and I talked about waiting for that but ultimately decided that one of the biggest advantages we can give our children is to grow up in a four-generation family filled with wonderful male and female role models that will be part of their daily life. While we are still young at only 35 years old, we want our children to know their grandparents, great-grandparents, and, in the case of Aunt Donna for whom this blog was started, their great, great aunt. We want them to be able to play with their cousins; to take family trips together. This means it’s time to start a family now. As such, we needed to use a donor egg to provide half of the DNA when creating the embryos. (Just as with opposite-sex couples who require the use of an egg donor, for same-sex male couples, the donor egg comes either from a female family member, a female friend, or an egg donation agency.)
To protect our privacy, the donor’s privacy, and our children’s privacy, we cannot discuss the source of our donor eggs. We will say that we found an incredible match who will serve as the egg donor for all of our children. It is difficult to express the love and gratitude we feel towards this person and their altruism. When the embryos are created, half will be fertilized with my DNA, half with Aaron’s DNA. This means all of the children will be genetically ours and be related to each other as either half or full genetic siblings. Our initial plan is to have four kids over the next five years, probably two boys and two girls.
For the purpose of explaining the process, we’ll assume that you are going to use an egg donation agency. An egg donation agency is a firm that specializes in finding, evaluating, and working with potential egg donors and Intended Parents. They bring the parties together, charge a fee for their services, and help coordinate the attorneys and IVF clinic orders so the process runs smoothly. Good egg donor agencies also work with psychologists to remove any potential egg donor who is motivated by money or economic need as they want the spirit truly to be an altruistic desire to help another family have children. For wealthy couples, other alternatives exist, such as using certain concierge services. For example, if you couldn’t find what you wanted at any given moment in an agency donor database – say you wanted an egg donor who had a degree from an Ivy League university and who participated in beauty pageants – it is still achievable.
 When signing up with an egg donation agency, the Intended Parents fill out a profile with their personal information. If accepted, they will receive credentials to access the agency’s proprietary database. Once inside the database, the Intended Parents will be able to search detailed listings of potential egg donors who want to help others have a baby. The good thing about egg donation in the United States is that, unlike sperm donors, egg donors often have extensive background information (a disparity that exists presumably because it requires more effort for an egg donation cycle to be completed than it does for a man to donate sperm). These database records will include photographs throughout the egg donor’s life, a detailed personal and family medical history, education information, a personal profile that often includes several essay questions, and more. Depending upon the agency, some of these profiles can run 50+ pages. Certain egg donation agencies allow the egg donor to put restrictions on the type of family she is willing to help. For example, an egg donor may decide that she does not want to donate to a same-sex married couple or a single woman. Be aware of this before potentially getting your heart broken during an emotional time.
When signing up with an egg donation agency, the Intended Parents fill out a profile with their personal information. If accepted, they will receive credentials to access the agency’s proprietary database. Once inside the database, the Intended Parents will be able to search detailed listings of potential egg donors who want to help others have a baby. The good thing about egg donation in the United States is that, unlike sperm donors, egg donors often have extensive background information (a disparity that exists presumably because it requires more effort for an egg donation cycle to be completed than it does for a man to donate sperm). These database records will include photographs throughout the egg donor’s life, a detailed personal and family medical history, education information, a personal profile that often includes several essay questions, and more. Depending upon the agency, some of these profiles can run 50+ pages. Certain egg donation agencies allow the egg donor to put restrictions on the type of family she is willing to help. For example, an egg donor may decide that she does not want to donate to a same-sex married couple or a single woman. Be aware of this before potentially getting your heart broken during an emotional time.
Once you have found the egg donor that you feel is the right choice, the process for proceeding varies depending upon the egg donation agency. Usually, it is around this time that you will need to complete an agreement with the egg donation agency called the “Agency Agreement”. This is the contract between the Intended Parents and the egg donation agency that clarifies its services, terms, prices, limits to liability, and other important conditions. You will need to get independent legal counsel to advise you during this stage, though it is usually common for large, reputable egg donation agencies to have a referral list of attorneys with whom they have worked frequently in the past.
After the agency contracts are signed, the egg donation agency will work on your behalf to coordinate with your fertility doctor and IVF clinic to arrange the necessary testing and monitoring to prepare the egg donor for the procedure. (More on that in a moment.) Prior to the egg donor taking any medication, it is important that a second contract, known as the “Direct Agreement”, be signed. The Direct Agreement is the contract between the Intended Parents and the egg donor. It lays out the terms and conditions on which they are entering into this agreement, much of which will be influenced by the laws of the state in which the contract is governed (which, in turn, will be determined by either the state of residence of the Intended Parents, the state of residence of the egg donor, or the state in which the egg donation procedure will occur at the IVF clinic). For example, in the United States, egg donation is an inherently altruistic act. While the egg donor will be compensated (unless dealing with a specialty arrangement, I believe medical ethics guidelines presently put the maximum recommended compensation at $10,000 per egg donation cycle as well as placing a lifetime restriction on egg donation cycles to no more than six but I’d have to check), this compensation is not for the eggs themselves as it must be paid even if the procedure results in no usable eggs being retrieved. Rather, the compensation is offered as an offset for the time, effort, inconvenience, lost wages, and potential pain and risks to which the egg donor is subjected herself on behalf of the Intended Parents. That is, she agrees to help you and even if it doesn’t work out, you still have to pay her for the inconvenience of her donation interrupting her life and putting her at risk (albeit extremely low risk).
The Direct Agreement will require the Intended Parents and the egg donor to make some decisions about the nature of their relationship in the future. In an “anonymous” donation, the egg donor wants to help a family have a child but everyone wants to remain anonymous so they are not part of each others’ lives. In a “known” donation, the egg donor and Intended Parents know each other’s full identities and the egg donor may even attend the child’s birthday parties or other family events. It truly is a case-by-case situation that is determined by the individual circumstances of the donation. Each family will be different. For example, it isn’t unusual for an anonymous donation agreement to include a provision that allows the child to send a letter indirectly to the donor through an intermediary if he or she is curious about some element of the donor’s past. Likewise, even in an anonymous donation, the child that is born may have pictures and background information about the egg donor so they know from their earliest memories how they were born and the story of their origins. The important thing is that the nature of the gestational surrogacy arrangement never be kept a secret so that as far back as they can remember, the child understands the details about how he or she was created. There should be no mystery about the experience and they should be free to ask whatever questions they feel they need to ask to understand it.
Finding the Right Fertility Doctor and IVF Clinic to Create Your Embryos
At the same time you were searching for an egg donor (if required), you were also looking for a fertility doctor and IVF clinic that you felt was right for you. For Aaron and me, this step was easy. He and I are scientifically-minded so we wanted the best outcomes. We also wanted someone who was motivated by helping build families because they truly love parenthood and babies. We researched IVF clinics throughout the United States and analyzed their success rates, which we defined as the number of healthy babies brought home by Intended Parents after completing the gestational surrogacy process. We attended the surrogacy conference I mentioned earlier, met with representatives from multiple IVF clinics, discussed those meetings and the literature they provided us, went back for a second round of interviews with our final choice via a Skype interview and then, ultimately, visited their clinic in person. For privacy reasons, I don’t want to mention the name of the clinic we are using (at least not at the moment) but I will say that we are absolutely, completely, and totally thrilled with them. Words cannot express how wonderful the staff is. We wanted a group of people who were not just concerned with us, the Intended Parents, but also the egg donor and the Gestational Carrier. They passed each and every one of our high standards with flying colors.
Our fertility doctor had us do the first round of testing in the Kansas City area to reduce our need to travel given how busy we are. First, he had our family physician conduct a physical examination. Then, we had to visit several laboratories so our blood, semen, and urine could be analyzed and tested for nearly every type of infectious disease and condition you can imagine. Once those results came back as perfect, we flew to the IVF clinic, where we:
- Spoke with our fertility doctor face-to-face and discussed our plan for building our family.
- Met with a genetic counselor, who did a detailed family history and explained that they would be taking more blood and looking at our DNA to determine if we were carriers for recessive diseases. They would then test our egg donor for the same recessive diseases to let us know if there was a compatibility problem. If that occurred, we would find another egg donor so as to effectively eliminate as much as mathematically possible the chances of our children being born with a particular disease.
- Met with a psychologist who evaluated us and offered to answer any questions about the process, including addressing any emotional concerns we had with it.
- Subjected ourselves to another round of the same blood, urine, and semen tests so the clinic had a double-set of negative results as per the FDA guidelines, ensuring that we were in perfect health with no medical issues, infections, or diseases.
- Walked through the process of creating the embryos.
- Walked us through the costs that would be billed to us by the IVF clinic.
- Donated the actual sample that will be used to fertilize the donor eggs on the day the embryos are created.
It was an exhausting, but emotionally rewarding, day. After it was all done, Aaron and I went out to a steakhouse and celebrated. At this point, we had been poked, prodded, tested, analyzed, and evaluated so much that we were glad it was mostly over on our end.
Once our egg donor was ready, our fertility doctor and IVF clinic sent remote orders to the egg donation agency with which we were working. The egg donation agency then setup the appointments for the egg donor at a local laboratory for her to go through many of the same things Aaron and I did. This includes a genetic analysis, to be compared to ours, to look at the compatibility of our DNA. The better IVF clinics are so strict on the genetic analysis that even if an egg donor is compatible with the Intended Parents, they may recommend the Intended Parents find an alternative egg donor because she might carry a handful of genes that simply correlate with higher later-in-life cancer risk. The theory is essentially, “you’re going through all of this trouble to give your kids the best advantages they can have in life, why not give them a significantly reduced risk of cancer, too?”.



Assuming everything goes well, the next step at this point in the gestational surrogacy journey is having the fertility doctor put the egg donor on a custom-tailored medical program designed to cause her body to develop and release more eggs than normal in a given cycle. The on-going monitoring is necessary to help ensure she does not experience adverse side-effects or produce too many eggs because you do not want her to suffer any fertility issues of her own years in the future. This involves using an ultrasound to look at the ovaries and determine the number of eggs that are developing. Egg quality is more important than egg quantity. Egg quality is largely determined by the age of the egg donor.
Creating and Freezing Your Embryos
On the day the egg donor is ready to donate her eggs to the Intended Parents, she brings a companion – usually her parent, her spouse, a sister or brother, or someone else close to her – to the IVF clinic. She is put under anesthesia and, in a matter of minutes, the fertility doctor retrieves the eggs. She wakes up shortly thereafter, and within one day should be back to her regular schedule. Within one to two weeks, her regular fertility cycle should resume.
When the developed eggs are retrieved by the doctor, the IVF clinic transfers them to a special fluid that is meant to simulate the inside of a woman’s reproductive system. In the case of a same-sex male married couple, the eggs are divided into two groups (this is known as a “split cycle”). Each egg is placed in a container with around 10,000 sperm from a frozen sample provided by one of the male Intended Parents. This means half of the eggs would be fertilized by one husband and half of the eggs by the other husband. Again, to clarify, all of the embryos would have the same female genetic donor, making each of the children full or half genetic siblings.
The next day, the medical staff removes the fertilized eggs from storage to see how they are developing. Usually, two circles are visible inside the fertilized egg, each representing the genetic contribution from the egg donor and the male Intended Parent who fertilized that specific egg. The embryos will be carefully watched over the next 5 to 6 days. During this process, some may not develop, or may cease developing, for seemingly no reason. For an additional cost, which practically all IVF patients at the better clinics opt to pay, the technology exists to biopsy a handful of cells from the edge of the egg towards the end of this development process. Essentially, 4 or 5 out of 200 cells are taken from what will become the placenta and analyzed for biological sex, chromosomal disorders, and genetic diseases.
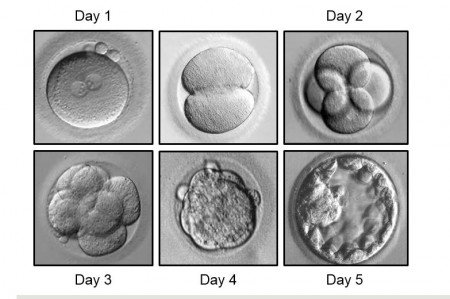 On the 6th day, the healthy embryos which pass the test are ready to be flash frozen in a process that halts metabolism so they can be revived when it is time to begin gestational surrogacy. At this point, they are made up of one of four categories.
On the 6th day, the healthy embryos which pass the test are ready to be flash frozen in a process that halts metabolism so they can be revived when it is time to begin gestational surrogacy. At this point, they are made up of one of four categories.
- The male embryos of male Intended Parent 1
- The female embryos of male Intended Parent 1
- The male embryos of male Intended Parent 2
- The female embryos of male Intended Parent 2
To make that clearer, in the case of Aaron and me, the four categories would be:
- Male embryos created with Joshua’s DNA
- Female embryos created with Joshua’s DNA
- Male embryos created with Aaron’s DNA
- Female embryos created with Aaron’s DNA
All embryos share the egg donor’s DNA for the female component.
(On a personal side note, and something I’m sure we’ll revisit many times in the future, it is not lost on us that all of this effort we’ve gone through results in our children having the genetic decked stacked in their favor. As we discovered during this process, both Aaron and I are extraordinarily fortunate in our genetics; a gift from God, the universe, or however you prefer to look at it. These advantages are compounded by the fact we are lucky enough to be born into a society where our intrinsic traits are largely given an unfair premium due to sociological and economic forces that happen to be dominant during our lifetime – e.g., we are roughly 6′ tall, white men with above-average cognitive ability, above-average social intelligence, and a willingness to defer gratification for better outcomes. We selected a genetic donor who also has wonderful personal traits – kindness and empathy were big ones to us – as well as great genetics. This genetic head-start is the first inheritance they will receive from us. It’s also, arguably, the most important as it will influence everything that ever happens to them. The societal implications for giving our babies this kind of advantage is something Aaron and I have discussed in private numerous times. We understand it may not be fair but, as future parents, how could we not do it? Why leave up to chance risks that could be neutralized or removed from before they take their first breath?)
Choosing a Gestational Surrogacy Agency
At this point, as far as the process of actually bringing the babies into the world, the egg donation agency and the egg donor have done their part. Now, you have these embryos, which are your genetic children. You need to find someone to whom you can entrust them for nine months while they grow into healthy babies. To do that, the best course of action is to find a highly-regarded, reputable gestational surrogacy agency in the United States. This agency finds women who are suitable Gestational Carrier candidates, has psychologists evaluate them, researches their past, does a home visit with a social worker, coordinates the gestational surrogacy process, and much, much more. The gestational surrogacy agency you choose is one of the most important decisions you’ll make. (As with the egg donation agency, when you are ready to hire the gestational surrogacy agency, they will have you sign an agency agreement with them. You need to have independent legal counsel look this over for you so you understand the details of the agreement into which you are entering.) Again, for privacy reasons, I’m not going to say which agency Aaron and I have chosen but I will say that, like everyone we ended up selecting, we knew after our first meeting with them they were the ones to whom we were going to entrust this task. A big part of that is the respect they showed for the Gestational Carriers.
Choosing a Gestational Carrier
The gestational surrogacy agency will spend six to twelve months searching for an appropriate Gestational Carrier for the Intended Parents. If you were to paint a picture of the typical Gestational Carrier selected by the better agencies in the United States, she tends to be a married, straight woman. She and her husband have two or more kids of their own, already, and do not want any more but they are highly altruistic. She loves being pregnant, has always experienced easy pregnancies with no complications, and, together, they decide this is something they want to do for another family. The Gestational Carrier’s husband and children are often an integral part of the process and become like extended family to the Intended Parents and their future children. Both he and she agree to remain celibate during part of the timeline, are tested for numerous diseases, subjected to background checks, analyzed by a psychologist, and visited by a social worker. One of the primary things the gestational surrogacy agency is seeking to avoid: they don’t want to work with women and families for whom economic need, or a desire for money, is the primary motivator. They want highly altruistic people for whom, yes, compensation is nice, but it is not the reason they and their family are doing this together. (The typical compensation for a Gestational Carrier in the United States tends to be between $40,000 and $60,000; an amount that isn’t even equal to minimum wage, let alone a livable wage, over the nine months she is entrusted with the Intended Parents’ child. Rather, it is meant to provide some comfort for the morning sickness, inconvenience, pain, and risk which she experiences due to her altruistic act. In fact, Intended Parents who believe that a Gestational Carrier is motivated by money should run, as quickly as possible, in the other direction.)
 During the matching process, the Intended Parents and Gestational Carrier will be brought together to meet face-to-face. Either can reject the match for any reason – or no reason at all – but the best gestational surrogacy agencies are so good at their job that a super-majority of their first placement recommendations are accepted by both parties.
During the matching process, the Intended Parents and Gestational Carrier will be brought together to meet face-to-face. Either can reject the match for any reason – or no reason at all – but the best gestational surrogacy agencies are so good at their job that a super-majority of their first placement recommendations are accepted by both parties.
Once a match has been made, the Gestational Carrier and Intended Parents negotiate a Direct Agreement between themselves. Depending upon the state laws under which the gestational surrogacy contract is being governed, this agreement will require specific language and protections for everyone involved. For example, it will require the Gestational Carrier to agree that she has no rights to the Intended Parents’ biological baby, but it also requires the Intended Parents to agree that they are the parents of the baby and must take responsibility for the child no matter what happens, including all medical costs; that the Gestational Carrier is not the baby’s mother, has no responsibility to the child, and is doing this as an altruistically-motivated act for the Intended Parents. The Gestational Carrier’s spouse will need to be a party to the agreement, too, because, in the case of a husband, he will need to also waive rights so he isn’t accidentally granted presumed paternity and find himself responsible for supporting the Intended Parents’ baby, to which he has no genetic relationship. Both the Gestational Carrier and her spouse, and the Intended Parents, will need to be represented by independent legal counsel.
Transferring the Intended Parents’ Embryo or Embryos to the Gestational Carrier
After all of this is done, the Intended Parents’ fertility doctor works with the Gestational Carrier to prepare her body to receive the Intended Parents’ embryo or embryos. On the day of the transfer, an embryo is brought out of cold storage and thawed. The doctor will attempt to implant the embryo or embryos on the lining of the Gestational Carrier’s uterus so it can continue developing.
The number of embryos transferred during any particular procedure will depend upon the probability of success, which is largely determined by the age of the egg donor at the time she donated the egg that created the embryo. Furthermore, in the case of a same-sex married male couple, many Intended Parents opt to implant two embryos, one from each genetic father, into the same Gestational Carrier so they can more easily afford building their family as they only have to pay for one pregnancy. While they will happily accommodate such a request, these days, the top-tier IVF clinics prefer to transfer only one embryo at a time for fertile same-sex couples because it reduces the chances of multiple pregnancies, which are associated with higher risks for both the babies and the Gestational Carrier. (After speaking with our doctor and the gestational surrogacy agency we intend to use, Aaron and I decided that the health of our Gestational Carriers and our babies is far more important than money. As a result, we will have two separate Gestational Carriers carry our first two children concurrently or near-concurrently so they are born about the same time. When this is done, the babies are referred to as “twiblings” in the fertility industry because they are approximately the same age with birthdays that are days, weeks, or months apart. We’re more than happy to pay double the expenses if it improves the odds that everyone ends up safe and happy. Later, when we go back to have our third and fourth children, we will repeat this same process.)
The Pregnancy Experience During Gestational Surrogacy
For the first trimester, the Intended Parents’ fertility doctor is responsible for monitoring the progress of the Gestational Carrier’s pregnancy. Thereafter, she is transferred to the care of her OB/GYN and the pregnancy proceeds completely as normal.
What Happens After the Gestational Carrier Gives Birth?
The next steps depend upon the state in which the gestational surrogacy occurs but, in a state such as California, during the pregnancy, a pre-birth order is attained that has both fathers listed as the two parents on the baby’s birth certificate. This protects both the Intended Parents and the baby, who is now the legally recognized child of both men, entitled to all of the protections and rights of any child. For example, if, God forbid, Aaron and I were hit by a proverbial bus the day before our babies were born, both babies would be entitled to inherit our estate as they would both be recognized as our children. Our parents would also be recognized as the legal grandparents, which provides further peace of mind in the event of an emergency.
When the time comes for the Gestational Carrier to give birth and return the baby to its genetic parents, the Intended Parents, the experience depends upon the hospital itself. In a state like California, there are delivery wards which have been built specifically for Gestational Carriers and Intended Parents. These suites consist of two adjoining rooms. That way, when the baby is born, the Gestational Carrier can recover with her husband or other family members in one room while the Intended Parents can bond with their baby and welcome visitors next door.
At this point, the Intended Parents are just the Parents. They take their baby home and raise it like any other parents. Depending upon the agreement with the Gestational Carrier, the Gestational Carrier may provide breast milk for several months by pumping her milk and providing it regularly to the baby or the baby may be put on formula, it depends entirely on the situation and the specifics of each child’s birth. One cool thing about the process is that it is fairly common for a Gestational Carrier to decide she wants to carry another sibling for the same family a year or two later. The emotional ties are already there with the Parents and the baby so going through the process again is natural and comfortable.
How Much Does Gestational Surrogacy Cost?
This is an incredibly difficult question to answer because every gestational surrogacy journey is unique. This means practically no two gestational surrogacy experiences will cost the same. Generally speaking, depending upon a wide range of factors, the process, start-to-finish, will probably cost somewhere from $85,000 to $150,000. If you are a married same-sex male couple, you’re probably best budgeting somewhere in the $125,000 range, give or take fifteen percent. While that is a lot of money, a married couple, both of whom have a bachelors degree, will earn an average of at least $4,600,000 over their lifetime on a combined basis. A married couple, both of whom have professional degrees in law, medicine, or engineering, might expect to earn an average of somewhere north of $8,000,000 over their lifetime on a combined basis. Like all things in life, it’s a matter of priorities. You work to live, not the other way around. If it is something that you and your spouse want, it is completely attainable.
The good new is that a large and ever-increasing percentage of employers now offer gestational surrogacy benefits to employees as a recruitment and retention strategy. IBM offers its employees up to $20,000 in surrogacy benefits to help off-set the costs. American Express offers 20 weeks of paid parental leave and up to $35,000 in surrogacy benefits. Starbucks offers both full and part-time workers up to $20,000 for IVF. Johnson & Johnson offers $35,000 a year for infertility treatments plus $20,000 in reimbursement for surrogacy. The Wall Street Journal took note of this new compensation strategy in a February 7, 2018 article called The Latest Way to Woo Workers: Fertility Benefits, stating that, “Some 66% of employers plan to offer fertility benefits by 2019, according to a January survey by advisory firm Willis Towers Watson PLC. That is up from 55% last year. The survey included around 400 companies with a total seven million workers. Of employers already offering financial assistance, 81% said the benefits would apply to same-sex couples next year, compared with 65% in 2017. Those boosting coverage cited wanting to diversify their ranks and to better recruit and retain people as their top reasons.”
What Have You Learned During the Gestational Surrogacy Journey?
This has been, and continues to be, an incredible experience. There are a few things that come to mind right away. In no particular order …
First, more than half of the people who go through this process are straight, married opposite-sex couples. Usually, they are both fertile but for some reason, the wife keeps miscarrying. Prior to this, I had no idea how common, and painful, this was. We’ve heard husbands and wives talk about losing five, six, seven or more babies during pregnancy and becoming despondent; about how they often don’t tell anyone and suffer in silence because there is a sense of shame. Because Aaron and I have been so open about our journey to parenthood in our day-to-day lives, many people – friends, acquaintances – have opened up and told us they secretly went through IVF or some other fertility treatment. The empathy I feel for them is deep. I just … I didn’t know. It was, and is, heartbreaking to me.
Second, I realized that men have a biological clock every bit as real as women. When ours activated, Aaron and I would find ourselves wandering through the baby section of a department store for twenty minutes without realizing it. We’d catch ourselves day dreaming about what our kids will be like; these little people that we have the privilege and gift to help guide into self-sufficient adults. It’s changed something internally. We’ve also found that it’s harder to read certain news stories if it involves a child being hurt. It’s these small things that you hear about but experiencing them first thing is different. On the flip side, we get so excited about the things we’re going to get to share with our kids. For example, we are having more fun than you can even imagine building their library. There are boxes of hardback book sets arriving constantly. It’s going to be incredible.
Third, we’ve always been driven and responsible but the idea of being responsible for these helpless lives entirely dependent upon us has caused Aaron and me to become almost hyper-focused on getting our lives and businesses simplified, streamlined, and firmly in place for what we hope will be the next 50+ years. When we think about Kennon-Green & Co., we feel, on a visceral level, that everything we do matters because not only have others entrusted their life savings to us, but this is the institution that will ultimately handle the wealth we’ve made from scratch; that we will hand down to our children, and our grandchildren, and our great grandchildren. There’s a sense of building things that live beyond our own lifetime that we always had but somehow, it more tangible to us now.
Fourth, I thought for a long time that my biggest concern would be raising kids that were still driven despite the affluence and privilege into which they are going to be born. I have peace with that now. I trust Aaron and my ability to raise kind, sensitive sons and daughters who never apologize for the blessings they have been given but do not take them for granted, either. This happened because of a conversation we had last summer with the husband of our Korean teacher. While over at their home for a “welcome back for the fall semester dinner”, he said something that was exactly what I needed to hear, at exactly the moment I needed to hear it. It changed my perspective entirely. I’m extremely grateful for that gift.
Some Final Thoughts on Gestational Surrogacy
For Aaron and I, we can’t say the exact timing, or where we are in the process, but we will say that, God willing and absent any unexpected surprises, we expect to have our first two kids by the end of next year. We’re rushing to finish the spin-up of the asset management firm before that time so it is a self-running, streamlined engine before we have to deal with midnight feedings and diaper changes. Still, we have little doubt that parenthood is going to be the best, most important, thing we will ever accomplish.
——–
All images and videos licensed from Shutterstock